
Glaucoma,Provider Newsletter,Uncategorized
According to the World Health Organization, glaucoma is the leading cause of preventable blindness worldwide. Glaucoma can be subdivided into two types based on anterior segment anatomy: open-angle glaucoma or angle-closure glaucoma. While open-angle glaucoma is the significantly more prevalent form of the two, angle-closure glaucoma is more likely to cause bilateral blindness.
Angle closure is broken down into a spectrum of conditions that involves narrowing of the anterior chamber angle. It can be thought of as a continuum that flows from primary angle closure suspect (PACS) to primary angle closure (PAC) to primary angle closure glaucoma (PACG). These conditions vary on the basis of amount of visible trabecular meshwork on gonioscopy, intraocular pressure, presence of peripheral anterior synechiae, and glaucomatous optic nerve damage.

Caption: A comparison of the angle closure spectrum from the 2016 American Academy of Ophthalmology Preferred Practice Pattern.
Patients on the angle closure spectrum are actually more common than you might think. One study has shown that almost 1 in 11 patients diagnosed with primary open angle glaucoma actually have angle-closure glaucoma. Moreover, almost 13% of patients referred for routine cataract surgery were found to have undetected PACS or PAC.
The risk factors for angle closure can be divided into anatomical and demographic subcategories.
Anatomical risk factors:
- Hyperopia
- Short axial length
- Shallow anterior chamber depth (peripheral or central)
- Steep corneal curvature
- Thick crystalline lens
- Ciliary body configuration (plateau iris)
Demographic risk factors:
- Chinese, Vietnamese, Pakistani, or Inuit descent
- Female gender
- Older age
- Family history of angle closure
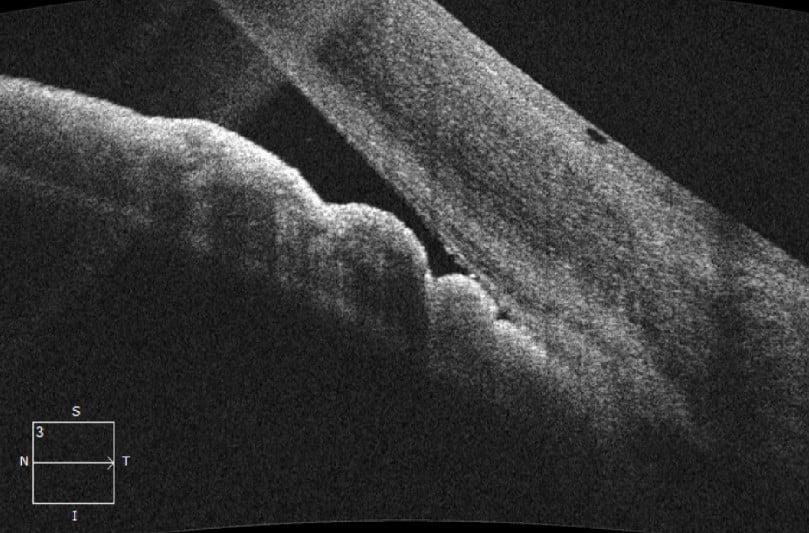
Caption: An anterior segment OCT showing a closed angle
Because of the significant morbidity associated with angle closure, it is important that these patients are identified and treated (if indicated). The three most common treatment options are YAG peripheral iridotomy, argon laser iridoplasty, and cataract surgery.
Laser Peripheral Iridotomy (LPI)
LPI is often considered the first line treatment for patients on the angle closure spectrum, particularly those with PAC or PACG. This relatively non-invasive technique involves creating a laser opening in the peripheral iris to equalize the pressure gradient between the posterior and anterior chambers, thus relieving any pupillary block. The Zhongshan Angle Closure Prevention Trial, or ZAP Trial, looked at the benefits of LPI in preventing patients with PACS from developing elevated intraocular pressure, peripheral anterior synechiae, or acute angle closure over a 72 month period. This trial found that the overall incidence of angle-closure disease was quite low but could be further reduced by performing a prophylactic LPI. Because of the relatively low incidence of outcomes that are not immediately sight threatening, the ZAP Trial recommended observation of PACS patients rather than prophylactic LPI. However, since LPI is a relatively low risk procedure, many ophthalmologists still offer LPI to PACS patients particularly if they have a high risk of progressing to PAC or PACG due to other risk factors (e.g., use of medications that can provoke an angle closure attack).
Argon Laser Iridoplasty
If LPI fails to produce significant deepening of the anterior chamber angle, as often is the case with plateau iris, argon laser iridoplasty may be indicated. Laser iridoplasty involves using low-level laser burns in the peripheral iris to create contraction of the stroma that pulls the iris tissue away from the angle. This is a great option for patients hoping to avoid more invasive interventions.
Cataract Surgery for Angle Closure
In the Effectiveness in Angle-Closure Glaucoma of Lens Extraction (EAGLE) study, researchers looked at the efficacy, safety, and cost-effectiveness of clear lens extraction versus laser peripheral iridotomy in the first-line treatment of PAC and PACG. They found that clear lens extraction showed greater efficacy and was more cost-effective than LPI, and thus recommended lens extraction as a first-line treatment. In light of this, it may be tempting to recommend lens extraction to all PAC and PACG patients. However, lens extraction is a higher risk procedure than LPI or iridoplasty, and also puts patients immediately into absolute presbyopia.
Sometimes all of the above options may be viable for a patient. In these cases it is even more important to discuss the risks and benefits of each procedure to help our patients come to an informed decision.
References:
Azuara-Blanco, Augusto, et al. “Effectiveness of Early Lens Extraction for the Treatment of Primary Angle-Closure Glaucoma (EAGLE): a Randomised Controlled Trial.” The Lancet, vol. 388, no. 10052, 2016, pp. 1389–1397., doi:10.1016/s0140-6736(16)30956-4.
He, Mingguang, et al. “Laser Peripheral Iridotomy for the Prevention of Angle Closure: a Single-Centre, Randomised Controlled Trial.” The Lancet, vol. 393, no. 10181, Mar. 2019, pp. 1609–1618., doi:10.1016/s0140-6736(18)32607-2.
Prum, Bruce E., et al. “Primary Angle Closure Preferred Practice Pattern® Guidelines.” Ophthalmology, vol. 123, no. 1, 2016, doi:10.1016/j.ophtha.2015.10.049.
Varma, Devesh K., et al. “Undetected Angle Closure in Patients with a Diagnosis of Open-Angle Glaucoma.” Canadian Journal of Ophthalmology, vol. 52, no. 4, 2017, pp. 373–378., doi:10.1016/j.jcjo.2016.12.010.

Author: Emily R. Freeman, OD, MS, FAAO
Specialties: Medical Eye Care
Mount Vernon & Bellingham Clinics
I was inspired to write about this topic after managing an unfortunate case of a young man that became legally blind due to untreated angle closure glaucoma. I feel incredibly lucky to work alongside such talented staff and doctors at Northwest Eye Surgeons and within the local optometric community. Along with our great team, I enjoy working with all types of glaucoma and cataract patients in an effort to maximize their visual potential and improve their quality of life.

