
bilateral papilledema,Provider Newsletter
A 30-year-old Caucasian female presented to her family eye doctor for a comprehensive eye exam including a soft contact lens evaluation. She had not had an eye exam for many years. Upon dilation it was observed that she had bilateral papilledema. The family eye doctor chose to refer her to our clinic for further evaluation.
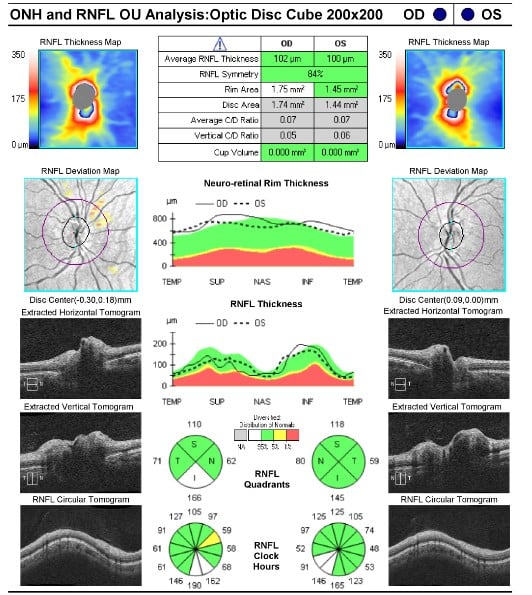
At our initial evaluation the patient showed the following:
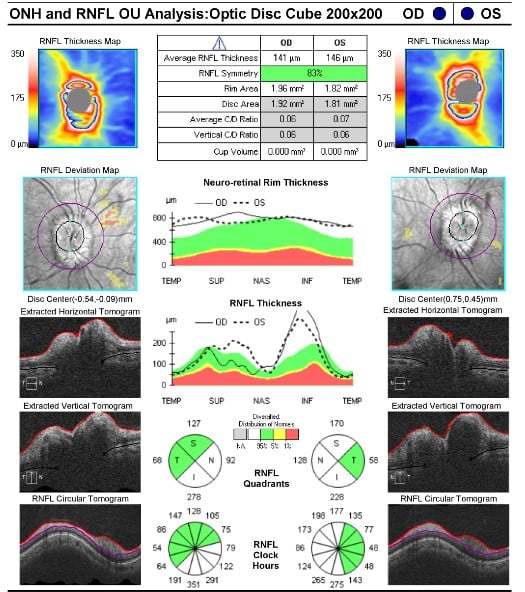
RNFL OCT was performed at this initial encounter confirming the bilateral papilledema noted upon exam (see image 1). Interestingly, upon careful questioning, the patient exhibited absolutely no symptoms related to papilledema. She had no history of head ache, no pain with ocular movement, no transient visual changes or blur, no diplopia. There was no indication of this concern prior to her presenting for her comprehensive examination with her family eye clinician.
Image 1 – RNFL OCT at initial evaluation.
Idiopathic Intracranial Hypertension (IIH) seemed the most likely differential considering bilaterality and that the patient was moderately overweight. The patient was not presently pregnant, nor was she currently or recently taking oral contraceptives, hormones, tetracycline derivatives, or corticosteroids – all of which have been shown to be associated with IIH1,2.
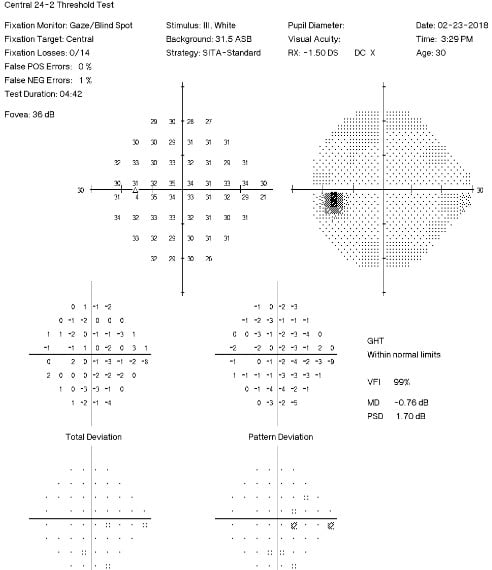
Visual field testing (see image 2 and 3) showed a very subtle enlarged blind spot OD, and mild non-pattern depressions OS. MRI with and w/out contrast of the brain and orbits was found to be normal other than evidence of papilledema.
Image 2 – OD Visual Field at early evaluation
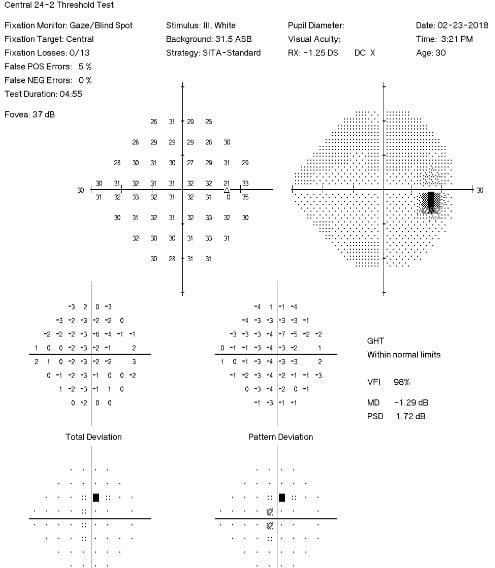
Image 3 – OS Visual Field at early evaluation
Considering that IIH can be self-limiting3, it was decided to not begin any form of treatment beyond monitoring and discussing weight loss. The patient was encouraged to pursue healthy options for reducing her current weight, then maintaining. The patient was encouraged to call if any visual or neurological symptoms developed.
What continued to be most fascinating in this particular case was the lack of any symptoms associated with the bilateral papilledema. The patient was monitored over the next 6 months during which time good reduction of papilledema was observed OU (see image 4). We have recommended she return to her family eye care doctor for continued monitoring.
Image 4 – RNFL OCT 6 months after initial presentation
1) Kanner LA, Klein J, Gaffar M, Pomeranz H, Frank G. (2018). New-Onset Isolated Asymptomatic Papilledema in Two Patients Treated With Recombinant Growth Hormone. Clinical Pediatrics. 57(4):471-474.
2) Rigi M, Almarzouq S, Morgan M, Lee A. (2015) Papilledema: epidemiology, etiology, and clinical management. Eye and Brain. 7:47–57.
3) Bidot S, Bruce BB, Saindane AM, Newman NJ, Biousse V. (2015). Asymmetric papilledema in idiopathic intracranial hypertension. Journal of Neuroophthalmology. 35(1):31-36.
 Author: Justin L. Wright, OD
Author: Justin L. Wright, OD
Bellingham and Mount Vernon clinics
I continue caring for patients in our Mt. Vernon and Bellingham offices. I enjoy seeing patients have a wonderful visual outcome following cataract surgery, this makes work exciting and rewarding. My wife and I are entering a new stage of life as our oldest daughter graduates from High School this year and moves off to college. Our 3 boys still at home keep us hopping.

