
Ali S. Mainayar, OD
For years, the standard answer for “gritty” or “burning” eyes was a simple bottle of artificial tears. For many of my patients though, those drops feel like pouring water into a leaky bucket, the relief is gone in minutes. Over the years of treating advanced dryness, I’ve learned that we cannot fix “dry” eyes until we address the inflammation and oil quality that keep the surface of the eye protected.
If you’ve been told you have dry eye, you are likely part of the 86% of cases caused by Meibomian Gland Dysfunction (MGD). This is often driven by a common but underdiagnosed condition: Ocular Rosacea.
The Root of the Problem: Ocular Rosacea and MGD
Most people think of rosacea as a skin condition that causes facial flushing. However, about 80% of rosacea patients also suffer from ocular manifestations. In these cases, tiny abnormal blood vessels (telangiectasia) develop along the eyelid margins. These vessels leak inflammatory markers directly into the Meibomian glands.
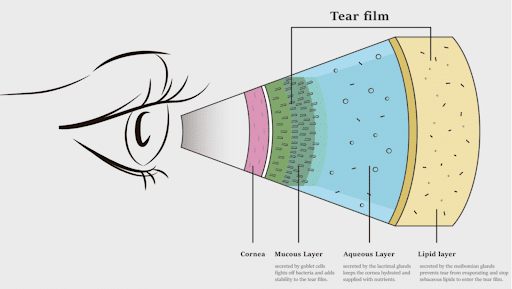
When these glands become inflamed, the oil (meibum) changes from a healthy, olive-oil consistency to something more solidified like toothpaste. This leads to:
- Blocked Glands: The thick oil can’t escape.
- Tear Film Instability: Without a healthy oil layer, your watery tears evaporate almost instantly.
- The “Watery Eye” Paradox: Your eyes may actually water more as a reflex to the underlying dryness, but these tears lack the “stickiness” needed to stay on the eye.
A Breakthrough Solution: Intense Pulsed Light (IPL)
While warm compresses and lid scrubs help, they often don’t reach the deep-seated inflammation caused by ocular rosacea. This is where Intense Pulsed Light (IPL) has changed the game.
Originally used in dermatology, IPL uses specific wavelengths of light to target the abnormal blood vessels around the eyes. The benefits are fourfold:
- Reduces Inflammation: It closes the “leaky” vessels that feed inflammation to the glands.
- Liquefies Meibum: The gentle heat helps melt the hardened oils, making them easier to express.
- Eradicates Bacteria/Mites: It reduces the load of Demodex mites and bacteria that contribute to eyelid irritation.
- Restores Stability: By improving oil quality, we significantly increase “Tear Breakup Time” (TBUT), the clinical measurement of how long your tear film stays intact between blinks.

What the Science Says
Recent studies have confirmed the power of this interventional approach. A 2025 study published in Nature demonstrated that patients receiving a series of IPL sessions showed superior long-term improvements in non-invasive tear break-up time and meibum quality compared to those using traditional methods alone. Furthermore, research from the Mayo Clinic has shown that up to 89% of patients with refractory dry eye (those who didn’t get better with other treatments) experienced significant symptom relief after a series of four IPL treatments.
The Path to Relief
Treating dry eye is a marathon, not a sprint. A typical protocol involves 4 sessions spaced a few weeks apart. Most of my patients notice a “turning point” after the second or third session, where they find themselves reaching for their drops less and less.
If you are tired of the constant “gritty” feeling and want to move beyond temporary fixes, it may be time to look at the health of your glands and the stability of your tear film.
About the Author
I chose to specialize in dry eye because I saw how much it impacted my patients’ quality of life—from struggling to work on a computer to losing the ability to wear contact lenses comfortably. What I find most rewarding is seeing the “aha!” moment when a patient finally gets relief after years of trying every drop on the shelf. Here at Northwest Eye Surgeons, I’m passionate about using the latest technology, like IPL, to provide interventional care that actually changes the trajectory of the disease.
References
- Lemp, M. A., et al. (2012). “Distribution of Aqueous-Deficient and Evaporative Dry Eye in a Clinic-Based Patient Cohort.” Cornea. (The landmark study establishing that 86% of dry eye is caused by MGD).
- Toyos, R., et al. (2015). “Intense Pulsed Light Treatment for Dry Eye Disease Due to Meibomian Gland Dysfunction.” Photomedicine and Laser Surgery. (One of the primary studies validating IPL for ocular use).
- Seo, K. Y., et al. (2025). “Long-term Efficacy of Intense Pulsed Light in the Management of Ocular Rosacea and Tear Film Stability.” Nature: Scientific Reports. (Recent data supporting long-term tear break-up time improvements).
- Dell, S. J., et al. (2017). “Comparison of Combined Intense Pulsed Light and Meibomian Gland Expression versus Meibomian Gland Expression Alone.” Clinical Ophthalmology. (Demonstrates why the interventional “light” approach is superior to traditional heat alone).
- Arita, R., et al. (2018). “Therapeutic Efficacy of Intense Pulsed Light in Patients with Refractory Meibomian Gland Dysfunction.” Ocular Surface. (Evidence of relief for patients who have failed other treatments).

